

Abstract
Background
Internal tandem duplication (ITD) mutation of the FMS-like tyrosine kinase-3 (FLT3) receptor gene occurs in about 25% patients with acute myeloid leukemia (AML) and confers a poor prognosis. Several studies have reported that a higher mutant allelic burden is associated with a worse prognosis.
Methods
Adult patients with FLT3-ITD mutated AML treated at our institution from January 2001 to January 2018, who had quantified FLT3-ITD allele burden, were identified. Patients with acute promyelocytic leukemia and core-binding factor AML were excluded.Patients were assigned into 2 groups; Group 1 included patients who received idarubicin and cytarabine (IA) containing induction and Group 2 included patients who received sorafenib in addition to IA containing regimens at induction.
Mutant allelic burden was expressed as the ratio of area under the peak of mutant allele to total FLT3. Relapse free survival (RFS) for patients achieving complete response (CR)/CR with incomplete recovery (CRi) was defined as time from CR/CRi to relapse or death. Overall survival (OS) was defined as time from treatment to death. Patients were censored at last follow up. Time from therapy to allogeneic hematopoietic cell transplant (AlloHCT) was handled as a time-dependent variable. The optimal cutoff of mutant FLT3-ITD allelic burden was defined as the cutoff to divide the whole cohort with the highest statistical significance.
Results
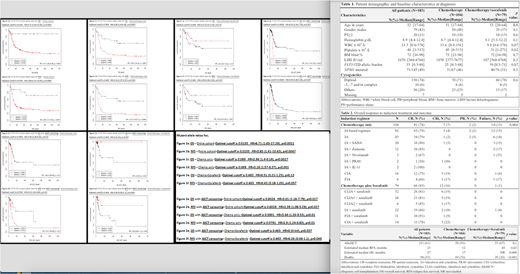
A total of 183 patients withFLT3-ITD mutated AML were identified including 104 (57%) in Group 1 and 79 (43%) in Group 2. Baseline characteristics are summarized in Table 1. The median age was 52 years (range, 17-64). The median allelic burden of mutant was 33% (range, 0.3% to 88%). This was comparable between the two groups (p=0.6). The CR/CRi rates following induction for Group 1 vs Group 2 were 85% vs 99%, respectively (p=0.004). Overall, 111 (61%) patients received an AlloHCT, at any time during the follow up, more frequently in Group 2 than in Group 1 (67% vs 56%, respectively, p=0.1). The median RFS for Group 1 and 2 were 12 and 45 months, respectively (p=0.02); the median OS was 17 months in Group 1 and has not been reached in Group 2 (p=0.008) (Table 2).
The optimal mutant allele burden cutoff for OS and RFS in the entire cohort was 1.55% (p=0.002) confirming the adverse effect of FLT3-ITD even at low level. The cutoff was 6.9% in Group 1, with no optimal cutoff value in Group 2 (Figure 1) confirming the value of sorafenib inFLT3-ITD mutated AML. When censored for AlloHCT; the FLT3-ITD cutoff for OS and RFS was 60% and 60% in the entire group. For Group 1 the cutoff values where 59% and 7.9% for OS and RFS, respectively. For Group 2 the cutoff values were 46% and 46%, respectively (Figure 2).
On multivariate analysis, AlloHCT (HR 0.52; 95%CI 0.33-0.82; p=0.005), sorafenib (HR 0.6; 95%CI 0.38-0.93; p=0.02) and white blood cell count (HR 1.005; 95%CI 1.002-1.009) were independent predictors of OS with no impact by cytogenetics, concurrent NPM1, TP53, FLT3-D835 mutations or the FLT3-ITD allelic burden.
Conclusion
Although a higher FLT3-ITD allele burden is associated with a worse RFS and OS in patients with FLT3-ITD mutated AML treated with IA-based chemotherapy, it is no longer prognostic when sorafenib is added to the therapeutic regimen. Addition of sorafenib to intensive chemotherapy as well as AlloHSCT are associated with a significant improvement in OS on multivariate analysis.
Kadia:Novartis: Consultancy; BMS: Research Funding; Takeda: Consultancy; Celgene: Research Funding; Celgene: Research Funding; Jazz: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Takeda: Consultancy; BMS: Research Funding; Abbvie: Consultancy; Pfizer: Consultancy, Research Funding; Jazz: Consultancy, Research Funding; Novartis: Consultancy; Amgen: Consultancy, Research Funding; Abbvie: Consultancy. Sasaki:Otsuka Pharmaceutical: Honoraria. Daver:BMS: Research Funding; ImmunoGen: Consultancy; Karyopharm: Consultancy; Sunesis: Research Funding; Novartis: Consultancy; Otsuka: Consultancy; Karyopharm: Research Funding; Novartis: Research Funding; Daiichi-Sankyo: Research Funding; Pfizer: Research Funding; Incyte: Research Funding; Sunesis: Consultancy; Pfizer: Consultancy; Incyte: Consultancy; ARIAD: Research Funding; Alexion: Consultancy; Kiromic: Research Funding. DiNardo:Medimmune: Honoraria; Bayer: Honoraria; Abbvie: Honoraria; Celgene: Honoraria; Agios: Consultancy; Karyopharm: Honoraria. Pemmaraju:Affymetrix: Research Funding; SagerStrong Foundation: Research Funding; plexxikon: Research Funding; daiichi sankyo: Research Funding; samus: Research Funding; celgene: Consultancy, Honoraria; abbvie: Research Funding; cellectis: Research Funding; stemline: Consultancy, Honoraria, Research Funding; novartis: Research Funding. Short:Takeda Oncology: Consultancy. Bose:Astellas Pharmaceuticals: Research Funding; Incyte Corporation: Honoraria, Research Funding; Celgene Corporation: Honoraria, Research Funding; CTI BioPharma: Research Funding; Blueprint Medicines Corporation: Research Funding; Pfizer, Inc.: Research Funding; Constellation Pharmaceuticals: Research Funding. Cortes:Daiichi Sankyo: Consultancy, Research Funding; Astellas Pharma: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Arog: Research Funding; Novartis: Consultancy, Research Funding. Ravandi:Macrogenix: Honoraria, Research Funding; Seattle Genetics: Research Funding; Seattle Genetics: Research Funding; Sunesis: Honoraria; Macrogenix: Honoraria, Research Funding; Bristol-Myers Squibb: Research Funding; Amgen: Honoraria, Research Funding, Speakers Bureau; Amgen: Honoraria, Research Funding, Speakers Bureau; Jazz: Honoraria; Orsenix: Honoraria; Sunesis: Honoraria; Orsenix: Honoraria; Abbvie: Research Funding; Jazz: Honoraria; Bristol-Myers Squibb: Research Funding; Abbvie: Research Funding; Xencor: Research Funding; Astellas Pharmaceuticals: Consultancy, Honoraria; Xencor: Research Funding; Astellas Pharmaceuticals: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal